
More Information
Submitted: July 06, 2024 | Approved: July 13, 2024 | Published: July 15, 2024
How to cite this article: Shahine DE. Procedure for Determining Root Canal Length in Endodontics: A Mathematical Approach. J Clin Adv Dent. 2024; 8(1): 020-023. Available from: https://dx.doi.org/10.29328/journal.jcad.1001042.
DOI: 10.29328/journal.jcad.1001042
Copyright License: © 2024 Shahine DE. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Dental implants; “Shahine” formula; Dental radiographs

Procedure for Determining Root Canal Length in Endodontics: A Mathematical Approach
Dott Edward Shahine*
Libero Professionista in Legnago (VR), Italy
*Address for Correspondence: Dott Edward Shahine, Libero professionista in Legnago (VR), Italy, Email: [email protected]; [email protected]
Intraoral and extraoral radiographic investigations play a fundamental role in all dental disciplines. For endodontic treatment it is necessary, in addition to measuring with apex locators, also various radiographs in the preoperative, operative, and final control phase.
Even in surgical practice, and especially in implantology, the radiographic investigation remains essential to limit errors or complications.
The mathematical approach for the determination of the length of work in endodontics is a simple and costless procedure. This work intends to expose the reasons why it should, in certain cases, be taken into consideration.
The working length in endodontics
In endodontics, it is important to determine the working length to establish the exact apical extension of the instrumentation and the apical level of the root canal filling.
Mistakes made at this stage, both in excess or deficiency, will have repercussions negatively on the outcome of the treatment [1-3]. The apical limit must not be exceeded so as not to interfere with the healing process [4].
Overcoming the working length could cause perforation of the apex and periapical irritation due to its over-instrumentation, and infiltration of irrigating substances in the surrounding periodontal tissue due to the consequent overfilling. The result could cause an increased incidence of postoperative pain and a prolonged healing period, as a consequence of incomplete regeneration of the cement, the periodontal ligament, and the alveolar bone. If, instead, the working length is shorter, the instrumentation could be incomplete with insufficient filling of the root canal. Consequently, in the most apical portion, fragments of pulp would remain vital or necrotic, and this could cause postoperative pain or be responsible for the failure of the endodontic therapy [5-8].
The determination of the working length
There are different methods to determine the length of work, such as the knowledge of anatomy, the use of anatomical averages, tactile sensation, radiographic evaluation, or measuring with a cone of paper, to evaluate the limit between dry canal space and moist periapical region [9,10]. The determination of work length using the radiographic technique was introduced in 1899 when C. Edmund Kells initiated the clinical use of X-rays in Dentistry.
The accuracy of length measurement working with the radiographic method depends on the particular radiographic technique applied [11]. It presents some limits associated, on the one hand, with the technique itself and, on the other, with the patient. Generally, several intraoral radiography in the preoperative, operative, and final control phases are used, through a centering device and by the parallel axes technique. The perfect parallelism between the film and tooth axis and the perfect perpendicularity of the ray must be respected, to avoid the image of the tooth lengthens and gets deformed. The X-ray in traditional intraoral therapy has proven itself to be more faithful in reproducing correctly the dimensions of the dental elements, although it also usually highlights a slight magnification, which can be estimated in 3.4% for the anterior teeth, in 5.38% for premolars and 5.3% for the posteriors [12-20].
The limits of radiographic technique
The inaccuracies of the radiographic technique are well documented in the literature. It was detected that a file introduced into the root canal and diagnosed as short, compared to the radiographic apex, is extended beyond the tip of the root into the 33% of cases where X-ray had been performed with the bisector technique, and in 20% of cases in which it had been used parallel ray technique [21]. Stein, et al. [12] found that the radiographic distance of the file from the apical vertex was 0.7 mm shorter than the actual location of the file, and suggested that the working distance from the apical vertex should be smaller between 1.5 and 2.0 mm, to prevent the over instrumentation of the canal. Numerous studies have shown therefore that the canal length, determined radiographically, varies considerably compared to the effective value [11,22-24].
Apex locators
The endodontist who uses only X-rays may therefore frequently run into errors. Although they constitute a critical and integral part of endodontic therapy, there is a need to reduce exposure to ionizing radiation whenever possible [25,26]. For these and other reasons, apex locators have been introduced, performing a role of primary importance in this field [9]. They are accurate, fast, and easy to use, and in 85% of cases, they allow to carry out, at a minimum, one less X-ray [27]. However, apex locators cannot be considered a definitive alternative to traditional intraoperative radiographs, which represent the only way through which the endodontist can obtain guidance on the complexity of the canal anatomy [28].
The mathematical approach
The mathematical approach contributes to improving measurement accuracy and allows a further reduction of the number of intraorals, especially in those patients where the use of X-rays is non-indicated.
The mathematical hypothesis
When you insert a tool into a root canal, it results in close contact with all anatomical structures of the tooth itself. It is plausible to suppose that the instrument goes up, quantitatively and qualitatively, towards the same radiographic deformation of all structures around it.
The different elements that undergo in equal measure a radiographic effect can be compared metaphorically to as many current bank accounts subjected to the same rate of interest.
The “Shahine” formula
The report between the length of a root canal instrument inserted and the length of its projection must be identical to the report between the actual length of the tooth versus its projection on the X-ray. This leads us to the elementary mathematical reasoning of the proportions, which consists of the equality between two relationships, expressed in the formula:
x:y = c:d
In our case:
* x is the real canal length (the unknown for us).
* y is the length of x projected onto the radiography. It can be measured directly on the intraoral radiography.
* c is the length of the instrument inserted into the root canal while taking the intraoral X-ray
* d is the length of the instrument projected on the radiography.
The solution of the formula is
x = c X y/d.
The author suggests creating an Excel file with this formula and saving it. To find the real length of canal roots of interest it is sufficient to fill the three known requested parameters (length of the instrument, the length of its projection on the ray, and that of the root canal of our interest).
Our experience
In our daily practice, X-ray instruments and apex locators are utilized, assisted frequently by our mathematical formula. This helps us to obtain precise measures of anatomical structures of our interest, mainly root canal lengths.
When old patients return to our clinic for an endodontic treatment, we can search in our archive for their recent intraoral X-ray radiographs. In this case, we found that in the past we inserted a 10 mm implant (Figure 1). We measure its projection on the radiograph, the projection of the canal root length we need to treat, and through our formula, we can obtain the actual root canal length.
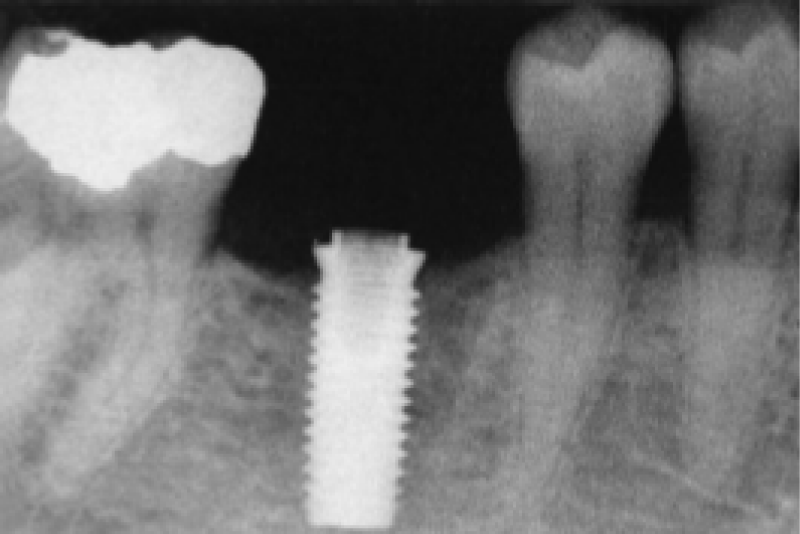
Figure 1: Intraoral Radiograph with an implant integrated with titanium that can be used as a metallic object for the calculation of root canal length.
In this case, we utilize a canal instrument (Figure 2) to calculate the real root canal length. The instrument’s length is a known value, thus, we measure its projection and that of the root canal, and through the proposed formula, we can obtain the real root canal length.

Figure 2: Intraorally Radiograph with an instrument inserted.
The aim of this article is to help simplify our daily endodontic procedures by using a simple mathematical principle. It allows us to have precise and costless measurements of the canal roots and it permits us to reduce the number of intraoral X-rays, above all in situations where the use of X-rays should be limited, avoided, or contraindicated (pregnant patients, uncooperative patients such as children or disabled people, patients with strong gag reflex, with perforations and false hidden streets, confluent and atypical channels, presence of anomalous anatomical structures).
In all other so-called normality situations, the mathematical approach, for its ease of handling, the absence of costs, and, above all, its harmlessness, could be taken into consideration as an auxiliary and complementary technique for the determination of the working length in endodontics, in association with the apex locators and intraoral X-rays.
Conflict of interest: The author declares that there is no conflict of interest. The author declares that he has not received institutional funding for the present study.
- Strindberg LZ. The dependence of the results of pulp therapy on certain factors: an analytic study based on radiographic and clinical follow-up examinations. Acta Odontol Scand. 1956;14:21-28. Available from: https://www.scirp.org/reference/referencespapers?referenceid=3558185
- Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod 1988;14(7):346-351. Available from: https://doi.org/10.1016/s0099-2399(88)80196-1
- Cavalleri G, De Fazio P, Gerosa R, Menegazzi G, Salvinelli C. Ni-Ti endodontic instruments: comparative tests of two types of Ni-Ti files. G It Endod Q1 1996:6-11
- Laurichesse JM. Clinical endodontics. Masson: Milan, 1990
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am 1967:723-744. Available from: https://doi.org/10.1016/S0011-8532(22)03244-X
- Wing K, S€oremark R, Sairenji E. A roentgenographic method for rapid evaluation of x-ray machines. Oral Surg Oral Med Oral Pathol. 1968;25(6):822-830. Available from: https://doi.org/10.1016/0030-4220(68)90154-0
- White SC, Frey NW. An estimation of somatic hazards to the United States population from dental radiography. Oral Surg Oral Med Oral Pathol. 1977;43(1):152-159. Available from: https://doi.org/10.1016/0030-4220(77)90366-8
- White SC, Stafford ML, Beeninga LR. Intraoral xeroradiography. Oral Surg Oral Med Oral Pathol. 1978;46(6):862-870. Available from: https://doi.org/10.1016/0030-4220(78)90321-3
- Gordon MP, Chandler NP. Electronic apex locators. Int Endod J. 2004;37(7):425-437. Available from: https://doi.org/10.1111/j.1365-2591.2004.00835.x
- Inoue N, Skinner DH. A simple and accurate way to measuring root canal length. J Endod. 1985;11(10):421-427. Available from: https://doi.org/10.1016/S0099-2399(85)80079-0
- Forsberg J. Radiographic reproduction of endodontic “working length” comparing the paralleling and the bisecting-angle techniques. Oral Surg Oral Med Oral Pathol. 1987;64(3):353-360. Available from: https://doi.org/10.1016/0030-4220(87)90017-X
- Stein TJ, Corcoran JF. Radiographic “working length” revisited. Oral Surg Oral Med Oral Pathol 1992;74(6):796–800. Available from: https://doi.org/10.1016/0030-4220(92)90412-J
- Hession RW. Endodontic morphology. III. Canal preparation. Oral Surg Oral Med Oral Pathol. 1977;44(5):775-785. Available from: https://doi.org/10.1016/0030-4220(77)90387-5
- Badiello R, Bernardi T. Radiation risks in the dental practice. Modern Dentist. 1984;1:84–92.
- Biagini C, Mastronola V. The problem of radiation in odontostomatology. Modern Dentist. 1986:3.
- Marci F. Prevention of ionizing radiation in the dental practice. Part I. Dental Cadmos. 1988;66(10):17.
- Marci F. The prevention of ionizing radiation in the dental office. 2. Dent Cadmos. 1988;56(12):15. Available from: https://pubmed.ncbi.nlm.nih.gov/3255619/
- Benazzi A, Cucchi G, D'Arcangelo V. Ionizing radiation absorbed by the patient. Dental Cadmos 1991;59(7):.
- Castellucci A, Falchetta M, Sinigaglia F. Radiographic determination of the location of the apical foramen. G It Endod 1993;1:13.
- Belcastro S, Guerra M, Staffoni N. Use of the lead apron in dental practice. Dental Cadmos 1993;61(17).
- Chunn CB, Zardiackas LD, Menke RA. In vivo root canal length determination using the Forameter. J Endod 1981;7(11):505-520. Available from: https://doi.org/10.1016/S0099-2399(81)80114-8
- Kuttler Y. A precision and biologic root canal filling technic. J Am Dent Assoc 1958;56(1):38–50. Available from: https://doi.org/10.14219/jada.archive.1958.0024
- Dummer PM, McGinn JH, Rees DG. The position and topography of the apical canal constriction and apical foramen. Int Endod J 1984;17(4):192-198. Available from: https://doi.org/10.1111/j.1365-2591.1984.tb00404.x
- Martínez-Lozano MA, Forner-Navarro L, Sánchez-Cortés JL, Llena-Puy C. Methodological considerations in the determination of working length. Int Endod J 2001;34(5):371-376. Available from: https://doi.org/10.1046/j.1365-2591.2001.00400.x
- Vertucci F. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics 2005;10:3-29. https://doi.org/10.1111/j.1601-1546.2005.00129.x
- Brunton PA, Abdeen D, MacFarlane TV. The effect of an apex locator on exposure to radiation during endodontic therapy. J Endod 2002;28(7):524-526. Available from: https://doi.org/10.1097/00004770-200207000-00009
- Pendlebury ME, Horner K, Eaton KA. Selection Criteria for Dental Radiography. 1st ed. London: Faculty of General Dental Practioners, Royal College of Surgeons of England. 2004;6-17. Available from: https://www.scirp.org/reference/referencespapers?referenceid=567728
- Soujanya; Muthu MS, Sivakumar N. Accuracy of electronic apex locator in length determination in the presence of different irrigants: An in vitro study. J Indian Soc Pedod Prev Dent. 2006;24(4):182-185. Available from: https://doi.org/10.4103/0970-4388.28074