
More Information
Submitted: August 07, 2024 | Approved: August 28, 2024 | Published: August 29, 2024
How to cite this article: Hugues JCO, Adorno CG. Rapid Upper Limb Assessment (RULA) and Rodgers Muscle Fatigue Analysis (RMFA) of Dentists using Optical Microscope, Loupes, or No Magnification during Endodontic Access: A Pilot Study. J Clin Adv Dent. 2024; 8(1): 024-028. Available from: https://dx.doi.org/10.29328/journal.jcad.1001043
DOI: 10.29328/journal.jcad.1001043
Copyright License: © 2024 Hugues JCO, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Rapid Upper Limb Assessment (RULA) and Rodgers Muscle Fatigue Analysis (RMFA) of Dentists using Optical Microscope, Loupes, or No Magnification during Endodontic Access: A Pilot Study
Juan Carlos Ortiz Hugues1* and Carlos G Adorno2
1Academy of Microscope Enhanced Dentistry (AMED), USA
2National University of Asuncion, School of Dentistry, Asunción, Paraguay
*Address for Correspondence: Juan Carlos Ortiz Hugues, DDS CEAS II AEP, Academy of Microscope Enhanced Dentistry (AMED), USA, Email: [email protected]
Dentistry is a challenging and demanding physical profession, and this impacts not only the quality of the task outcomes but also the professional’s quality of life.
The nature of dentistry demands prolonged static and awkward seated postures, frequent motions, positioning struggles, and working distances to the oral cavity for strategic procedure management, which become cumulative challenges over the working days, prone to discomfort, pain, or injuries, and musculoskeletal disorders for the operator.
The limitations of the naked eye in dentistry, particularly in terms of visual information and resolution, underscore the need for visual aids. These aids are crucial for achieving the precision required for accurate procedures. Also, visual aids, such as magnifying loupes and the operative microscope, have been in the market for a while, and their proper use has shown ergonomic benefits that promote a neutral working posture and changes in work practice-oriented to control unbalanced awkward posture and motions.
In this study, the Rapid Upper Limb Assessment RULA compares the posture between naked-eye dentistry, conventional loupes, and operative microscope, and with the observational assessment, determine the risk of developing musculoskeletal disorders and the need for priority of change. The Rodgers muscle fatigue analysis RMFA is used to predict fatigue in the muscular regions of the body during specific dental tasks.
Musculoskeletal disorders (MSD) are considered to be work‐related when the environment and performance of work contribute significantly to the condition; the condition is made worse or persists longer due to work conditions, or both. MSDs represent a significant occupational health problem among dental practitioners and have been attributed to deteriorating quality of life, often resulting in premature retirement and stress-related illnesses[1,2].
MSDs occurring among dental workers are chronic low back pain, tension neck syndrome, trapezius myalgia, and rotator cuff impingement [3,4].
The prevalence of general musculoskeletal pain in dental professionals (dentists and dental hygienists) ranges between 64% and 93% according to a systematic review [5]. Common MSDs affecting dental workers were neck, shoulder, and lower back [6,7].
Some studies have suggested that MSDs develop over time as a result of an incorrect working posture, and that being aware of these disorders and preventive practices early in professional life can minimize the risk of onset of MSDs [8]. Indeed, a correct posture promotes more energy, less stress and strain, less distraction from pain, and fewer errors; an incorrect posture results in pain, fatigue, poor work quality, negative attitudes, and aging [9].
Dental work processes are mostly predetermined, and these circumstances result in awkward body postures, which then require the dentist to work in constrained postures [10]. Dentists’ work includes several well-known risk factors for musculoskeletal symptoms in general and specifically for low back pain. The following widespread postures among dentists are considered risk factors: Forward bent sitting posture, accompanied by bending and twisting, and relative static work. Additionally, not only do the sitting and twisting postures have an effect on back pain, but the time spent in these postures greatly impacts musculoskeletal pain [11,12].
Neck pain has in fact been shown to be associated with any job where forward head posture is 20º or more for 70% of working time. On average, dentists and hygienists work with forward head postures of at least 30º for 85% of their time in the operatory. Poor posture, movement, or imbalances in the neck or shoulder can result in the three most prevalent pain syndromes seen in dentistry: tension neck syndrome, rotator cuff impingement or trapezius myalgia, pain, stiffness, movement difficulties, and tenderness are some of the symptoms related to this syndrome [13].
Neutral body posture during dental work should be a priority in dental education. During dental tasks, the dentist works in sitting postures, which are not designed for prolonged work. The neutral posture is attained when the body joints are the closest to the middle line of the body with ranges of motion parameters, assessed side view [14,15]:
- Head aligned to shoulders, shoulders aligned to hips, hips higher than the knees
- Head 0-20° downward
- Shoulder 0-25° forward
- Forearms 0-10° upward
- Hips 110-125° angulation
The operative microscope and magnifying glasses have been shown to improve the working postures in dentistry; new advances in the operative microscope with items such as the multifocal lens, binocular extender, and rotary ring, among others, designed to promote ease of use and ergonomic postural benefits, and the appearance of the ergonomic loupes with prisms inside the oculars deviating the view in angulations that promotes a neutral head posture while working are majors changes in the last years to improve performance, health and procedural outcomes in the operator [16].
The rapid upper limb assessment (RULA) is a survey method originally developed for ergonomic studies to assess working posture in workplaces where work-related upper limb disorders are reported [17]. The method uses diagrams of body postures and three scoring tables to provide an evaluation of exposure to risk factors. The Muscle Fatigue Analysis was proposed by Rodgers as a means to assess the amount of fatigue that accumulates in muscles during various work patterns within 5 minutes of work [18]. Based on the premise that a rapidly fatiguing muscle is more susceptible to injury and inflammation if fatigue can be minimized, so should injuries and illnesses of the active muscles. The purpose of the present pilot study was to evaluate the working position adopted during a standard endodontic procedure (endodontic access) with the Rapid Upper Limb Assessment (RULA) and Rodgers Muscle Fatigue Analysis (RMFA) tools.
In this preliminary study, endodontic access was performed in tooth number 4.7 (31 American system) by a specialist in endodontics using round and troncoconical burs attached to a highspeed handpiece.
The patients involved in the assessments were informed about the research project and signed an informed consent document.
A dental operating microscope (Newton SRL, Buenos Aires, Argentina), 2.5x Galilean conventional loupes or no magnification, i. e. the naked eye, were used on three different patients. All procedures were performed using an ergonomic chair (Dynamic model, Back Quality Ergonomics, The Hague, Netherlands) with telescopic and revolving armrests by the same operator, with 14 years of experience, 8 years of which were using the microscope. The operator reported no vision issues and no recent history of MSD. Each endodontic access procedure took between 8 – 10 min. A video camera was used to record the procedures from 3 different angles (2 lateral views (right and left) and a front view) in 3 different patients following the National Institute for Occupational Safety and Health (NIOSH) protocol for video recording jobs for risk factors. The position of the camera is standardized for all the recordings. The working posture adopted during the procedures was recorded by a video camera (Model STK-LX3, HUAWEI Technologies Co. Ltd., China) and evaluated using Rapid Upper Limb Assessment (RULA) and Rodgers Muscle Fatigue Analysis (RMFA) (Figure 1).
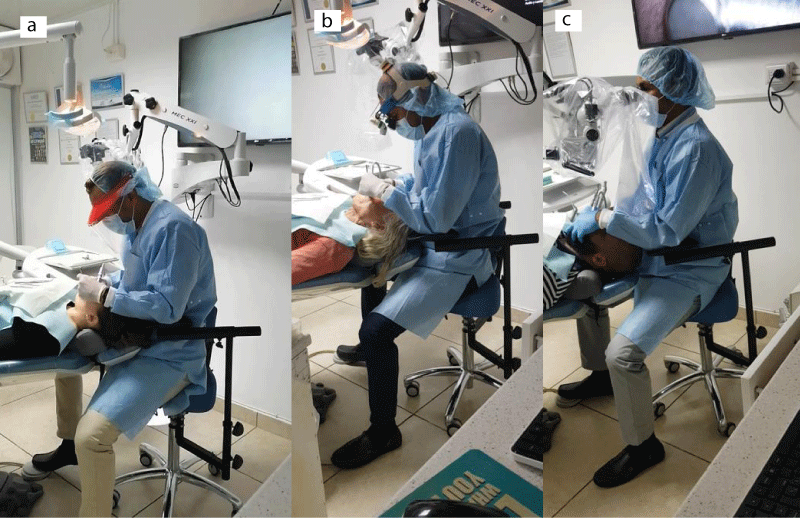
Figure 1: Postures a. Naked- Eye Dentistry b. Conventional 2.5 x Loupes c. Microscope Dentistry
The videos were analyzed by a Dentist and Certified Ergonomics Assessment Specialist, using the RULA and Rodgers muscle fatigue analysis sheets, observational assessing the parameters of both ergonomics assessment tools to screen postures, duration, and frequency risk modifiers when realizing the endo access task in the same teeth, with naked-eye, conventional loupes and the operative microscope.
The RULA considers the biomechanical and postural load requirements of job tasks/demands on the neck, trunk, and upper extremities. It uses a systematic process to evaluate the required body posture, force, and repetition for the job task being evaluated. The output of the RULA assessment tool is the final RULA Score, which is a single score that represents the level of MSD risk for the job task being evaluated.
The results determine the risk of work-related upper extremity disorders, help identify the muscular effort associated with working postures and excessive forces in static or repetitive work, and provide a simple scoring method with an auction-level output that identifies an indication of urgency (Figure 2).
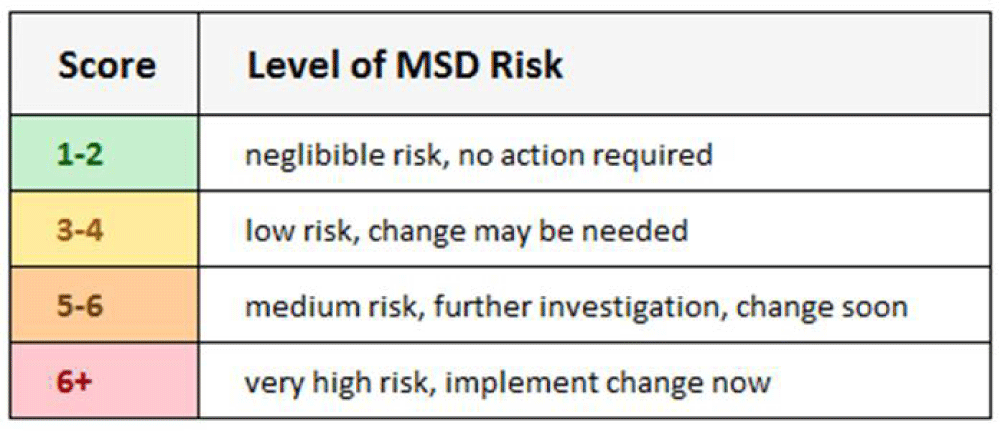
Figure 2: RULA level of MSD risk descriptions and cut points.
The RMFA analyzes the primary tasks performed (those done for more than 10% of the shift) and any tasks considered “difficult” for the task and each body region; the assessment will consider the three job risk factors by assigning each factor a rating by category.
The RMFA assessment tool provides a table that indicates the relative risk for fatigue within a category. The earlier the combination of categories is in the list, the lower the fatigue should be (i.e., it is better). The final score will depend on continuous effort, duration, and frequency combinations during the task to assess the amount of fatigue that accumulates in muscles during various work patterns within 5 minutes of work (Figure 3).
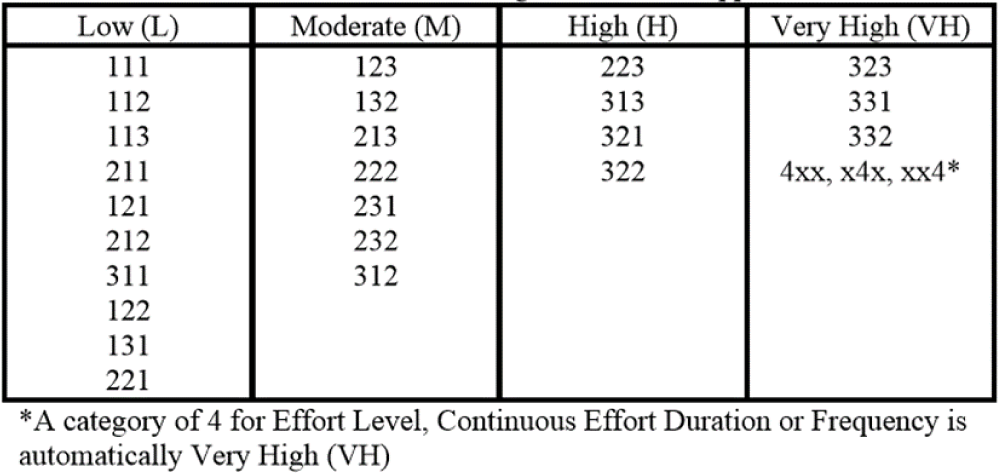
Figure 3: RMFA table provides an indication of the relative risk for fatigue within a category
Table 1 shows the detailed RULA scores of the working posture adopted during endodontic access of tooth 4.7 (31 American system) using the microscope, loupes, or no magnification.
| Table 1: Detailed RULA scores of theworking posture adopted during endodontic access of tooth 4.7 (31 Americansystem) using the microscope, loupes, or no magnification in three differentpatients. | ||||
| RULA item score | Microscope | 2.5× Loupes | No magnification | |
| Arm and wrist Analysis | Upperarm | 1 | 1 | 1 |
| Lowerarm | 2 | 2 | 2 | |
| Wristtwist | 1 | 1 | 1 | |
| Wrist | 2 | 3 | 3 | |
| PostureA | 2 | 3 | 3 | |
| Muscleuse | 1 | 1 | 1 | |
| Force/load | 0 | 0 | 0 | |
| Wristand Arm | 3 | 4 | 4 | |
| Neck, trunk, and leg analysis | Neck | 1 | 5 | 5 |
| Trunk | 1 | 4 | 4 | |
| Leg | 1 | 1 | 1 | |
| PostureB | 1 | 8 | 8 | |
| Muscleuse | 1 | 1 | 1 | |
| Force/load | 0 | 0 | 0 | |
| Neck,Trunk, Leg | 2 | 9 | 9 | |
| RULAScore | 3(Low risk, change may be required) | 6(Very high risk, implement change now) | 6(Very high risk, implement change now) | |
Very little difference in scores was observed during the arm and wrist analysis (Table 1). An operator ergonomic stool was used during the procedures and may have influenced the wrist and arm scores. During the three working conditions, the upper arm was positioned between 20-45 degrees forward from the shoulder, without abduction, and supported by the operator’s stool. The lower arm was positioned 60-100 degrees upward, where the most dynamic movement was in the wrists scores due to the continuous work with the handpiece in the right hand and holding the mirror in the left hand, both with bending and twisting. The use of arm supports has been reported to reduce static and median neck/shoulder activity, but not affect peak muscle activity [19].
The largest difference was observed during the neck, trunk, and leg analysis, in particular in the neck and trunk scores, which were lower for the working posture adopted during microscope use than for loupes and no magnification (Table 1). When using the microscope, the neck, trunk, and leg positions remained steady during the complete task cycle with low scores in their positions, without any bending or twisting. This is because the microscope allows the operator to adopt an upright sitting position whilst the focusing range of 200–415 mm can be continuously adapted to the requirements of the task [19]. However, the use of loupes or no magnification both resulted in the 20 degrees forward head posture neck position, with twisting and side bending. A cohort study that there was an increased risk of neck pain for people working with the neck at a minimum of 20°of flexion for more than 70% of the working time [20]. The trunk was observed to be forward bending up to 20 degrees with twisting and side bending and the legs well supported on the floor. A prolonged static posture was observed for all working conditions.
The use of conventional loupes and no magnification achieved similar scores. Thus, the overall RULA score was lowest for microscopes. By identifying the muscular effort that is associated with working postures and excessive forces while performing static or repetitive work, which may contribute to muscle fatigue. These three cases show that during the endodontic access, the operator required less postural load with the microscope to do the same procedure, especially in the neck and back, where the dentist suffers most of the pain, discomfort, and injuries.
Concerning the RMFA, Table 2 shows the change priority at each region according to the use of microscope, loupes, or no magnification. The underlying hypothesis of Rodgers’s MFA is that a rapidly fatiguing muscle is more susceptible to injury and inflammation. There are three factors used in the assessment; effort level, continuous effort duration, and effort frequency. According to this study, the biggest risk factor in all the working conditions was the continuous effort duration. This means that a posture was held continuously for at least 20 s and many for more than 30 s. However, the effort level and frequency in all the muscle groups were light to moderate. The loupes are an additional weight attached to the operator’s forehead that already has to position his/her head at an angle of 20º forward. This should be considered when evaluating these results.
The nature of prolonged static seated postures in dentistry and the very high score for muscle fatigue priority in this scenario may show that is one of the complexities to deal with in dentistry.
Table 2. Rodgers muscle fatigue analysis overall priority scores of each region according to the use of microscope, loupes, or no magnification.| Table 2: Rodgers muscle fatigue analysis overall priority scores of each region according to the use of microscope, loupes, or no magnification. | |||
| Region | Microscope | 2.5× Loupes | No magnification |
| Neck | Very High | Very High | Very High |
| Shoulders | Very High | Very High | Very High |
| Back | Very High | Very High | Very High |
| Arms/Elbow | Low | Very High | Low |
| Wrists/Hands/Fingers | Moderate | Very High | Low |
| Legs/Knee | Very High | Very High | Very High |
| Ankles/Feet/Toes | Very High | Very High | Very High |
Access cavity preparation is the first step in a series of procedures in endodontic treatment because it can affect all subsequent procedures and also the outcome [21]. Clinically, this procedure can last approximately 5 - 10 min. However, the duration of root canal treatment is variable but usually is between 60 to 90 min per session. Endodontic work involves performing high-precision tasks with a limited range of motion (constrained postures) resulting in isometric muscle contractions, difficulties in direct visualization (which causes awkward posture), visual demands requiring static postures, repetitive tasks for long periods and high precision where the use of magnification is strongly recommended, sometimes in combination with the exertion of high forces and psychosocial stress from the complexities of endodontics tasks, which also triggers muscular tension [22,23].
By using both ergonomic assessment tools to evaluate the same videos, extensive data could be obtained. Both methods evaluate risk factors for the development of musculoskeletal disorders in static activities such as dentistry, one (RULA) with a tendency for postural analysis such as and the other (RMFA) with a tendency to muscle fatigue risk by zones according to the task being performed.
These preliminary results suggest that the working positions adopted, especially by the neck and trunk, and muscle fatigue risk of the arms, elbow, wrists, hands, and fingers during an endodontic procedure (access cavity preparation) are affected by the type of magnification being used. Additionally, there the RMFA suggests a very high priority of change for the three working conditions due to the prolonged static posture.
A limitation of this particular study was the use of an ergonomically designed stool, which may play a significant role in decreasing muscular activity and supporting the cervical and arms during the task.
Future studies can also assess the new ergonomic loupes on the market and compare them to other visual aids in dentistry.
The preliminary data gained in the present pilot study will guide the design of larger-scale studies performed on dentists and dental students.
- Burke FJ, Main JR, Freeman R. The practice of dentistry: an assessment of reasons for premature retirement. Br Dent J. 1997 Apr 12;182(7):250-4. Available from: https://doi.org/10.1038/sj.bdj.4809361
- Kumar M, Pai KM, Vineetha R. Occupation-related musculoskeletal disorders among dental professionals. Med Pharm Rep. 2020 Oct;93(4):405-409. Available from: https://doi.org/10.15386/mpr-1581 .
- Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. The Journal of the American Dental Association.2003:134(10): 1344-1350. Available from: https://doi.org/10.14219/jada.archive.2003.0048
- Shaik AR, Rao SB, Husain A, D'sa J. Work-related musculoskeletal disorders among dental surgeons: A pilot study. Contemp Clin Dent. 2011 Oct;2(4):308-12. Available from: https://doi.org/10.4103/0976-237x.91794
- Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009 Aug;7(3):159-65.Available from: https://doi.org/10.1111/j.1601-5037.2009.00395.x
- Gupta A, Ankola AV, Hebbal M. Dental ergonomics to combat musculoskeletal disorders: a review. Int J Occup Saf Ergon. 2013;19(4):561-71.Available from: https://doi.org/10.1080/10803548.2013.11077005
- Jaoude SB, Naaman N, Nehme E, Gebeily J, Daou M. Work-Related musculoskeletal pain among lebanese dentists: An epidemiological study. Niger J Clin Pract. 2017 Aug;20(8):1002-1009.Available from: https://doi.org/10.4103/njcp.njcp_401_16
- Sakzewski L, Naser-ud-Din S. Work-related musculoskeletal disorders in dentists and orthodontists: a review of the literature. Work. 2014;48(1):37-45. Available from: https://doi.org/10.3233/WOR-131712
- American Dental Association. An Introduction to Ergonomics: Risk Factors, MSDs, Approaches and Interventions. A Report of the Ergonomics and Disability Support Advisory Committee (EDSAC) to Council on Dental Practice (CDP). 2004.
- Ohlendorf D, Erbe C, Nowak J, Hauck I, Hermanns I, Ditchen D, et al. Constrained posture in dentistry - a kinematic analysis of dentists. BMC Musculoskelet Disord. 2017 Jul 5;18(1):291. Available from: https://doi.org/10.1186/s12891-017-1650-x
- Ohlendorf D, Erbe C, Hauck I, Nowak J, Hermanns I, Ditchen D, et al. Kinematic analysis of work-related musculoskeletal loading of trunk among dentists in Germany. BMC Musculoskelet Disord. 2016 Oct 18;17(1):427. Available from: https://doi.org/10.1186/s12891-016-1288-0
- Ratzon NZ, Yaros T, Mizlik A, Kanner T. Musculoskeletal symptoms among dentists in relation to work posture. Work. 2000;15(3):153-158. Available from: https://pubmed.ncbi.nlm.nih.gov/12441484/
- Kawtharani AA, Chemeisani A, Salman F, Haj Younes A, Msheik A. Neck and Musculoskeletal Pain Among Dentists: A Review of the Literature. Cureus. 2023 Jan 10;15(1):e33609. Available from: https://doi.org/10.7759/cureus.33609
- Valachi DB. Practice Dentistry Pain-Free: Evidence-based Ergonomic Strategies to Prevent Pain and Extend Your Career (1st edition). Posturedontics Press. 2008.
- Yoshida Y, Matsumura N, Yamada Y, Hiraga S, Ishii K, Oki S, et al. Three-dimensional alignment of the upper extremity in the standing neutral position in healthy subjects. J Orthop Surg Res. 2022 Apr 15;17(1):239. Available from: https://doi.org/10.1186/s13018-022-03113-5
- Bud M, Jitaru S, Lucaciu O, Korkut B, Dumitrascu-Timis L, Ionescu C, et al. The advantages of the dental operative microscope in restorative dentistry. Med Pharm Rep. 2021 Jan;94(1):22-27. doi: 10.15386/mpr-1662. Epub 2021 Jan 29. Available from: https://doi.org/10.15386/mpr-1662
- McAtamney L, Nigel Corlett E. RULA: a survey method for the investigation of work-related upper limb disorders. Appl Ergon. 1993 Apr;24(2):91-9. Available from: https://doi.org/10.1016/0003-6870(93)90080-s
- Rodgers SH. A functional job analysis technique. Occup Med. 1992 Oct-Dec;7(4):679-711. Available from: https://pubmed.ncbi.nlm.nih.gov/1411855/
- Bolderman FW, Bos-Huizer JJA, Hoozemans Marco JM. The Effect of Arm Supports on Muscle Activity, Posture, and Discomfort in the Neck and Shoulder in Microscopic Dentistry: Results of a Pilot Study. IISE Transactions on Occupational Ergonomics and Human Factors, 2017:5: 92-105. Available from: https://doi.org/10.1080/24725838.2017.1335659
- Ariëns GA, Bongers PM, Douwes M, Miedema MC, Hoogendoorn WE, van der Wal G, Bouter LM, van Mechelen W. Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occup Environ Med. 2001 Mar;58(3):200-7. Available from: https://doi.org/10.1136/oem.58.3.200
- Krapež J, Fidler A. Location and dimensions of access cavity in permanent incisors, canines, and premolars. J Conserv Dent. 2013 Sep;16(5):404-7. Available from: https://doi.org/10.4103/0972-0707.117491
- Morse T, Bruneau H, Dussetschleger J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work. 2010;35(4):419-29. Available from: https://doi.org/10.3233/wor-2010-0979
- Kogler L, Müller VI, Chang A, Eickhoff SB, Fox PT, Gur RC, Derntl B. Psychosocial versus physiological stress - Meta-analyses on deactivations and activations of the neural correlates of stress reactions. Neuroimage. 2015 Oct 1;119:235-51. Available from: https://doi.org/10.1016/j.neuroimage.2015.06.059