
More Information
Submitted: September 10, 2024 | Approved: September 17, 2024 | Published: September 18, 2024
How to cite this article: Masoud HZ. Distinguishing Traditional and Internal Craze Lines in Human Enamel. J Clin Adv Dent. 2024; 8(1): 029-039 Available from: https://dx.doi.org/10.29328/journal.jcad.1001044
DOI: 10.29328/journal.jcad.1001044
Copyright License: © 2024 Masoud HZ. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Crack; Craze lines; Dental enamel; Internal craze lines; Intraoral examination; Microscopy

Distinguishing Traditional and Internal Craze Lines in Human Enamel
Hassan Zadeh Masoud*
Biomimetic Restorative Dentist, De Tandwachters, Moleneind ZZ 127, 9203 ZX, Drachten, The Netherlands
*Address for Correspondence: Hassan Zadeh Masoud, Biomimetic Restorative Dentist, De Tandwachters, Moleneind ZZ 127, 9203 ZX, Drachten, The Netherlands, Email: [email protected]
Objectives: This study aims to introduce and differentiate between traditional craze lines and a newly identified type of line in enamel, termed an “internal craze line.” This novel classification enhances diagnostic precision and carries significant clinical implications for treatment strategies. The goal is to provide a clear description of these two types of lines, discuss their unique clinical implications, and highlight their differing appearances and staining characteristics, contributing to improved understanding and management of enamel anomalies.
Method and materials: Four extracted teeth exhibiting visible and internal craze lines were selected and examined using a stereo microscope to observe the structural characteristics of the lines. Cross-sections of the coronal parts of the teeth were prepared to document the differences between traditional craze lines (extending from the dentin-enamel junction [DEJ] to the enamel surface) and internal craze lines (originating at the DEJ but terminating midway through the enamel). Additionally, intraoral observations were conducted under high magnification to identify the visual differences between the two types of lines, noting that traditional craze lines can be stained while internal craze lines cannot.
Results: Microscopic examination revealed two distinct types of lines: traditional craze lines extending from the DEJ to the enamel surface and internal craze lines terminating within the enamel. Intraoral observations confirmed that these lines could be distinguished under high magnification. Traditional craze lines appear as continuous lines reaching the enamel surface and can be stained, whereas internal craze lines are shorter, do not extend to the surface, and cannot be stained.
Conclusion: The identification of internal craze lines presents significant clinical implications. Differentiating between traditional and internal craze lines can enhance diagnostic accuracy and inform treatment decisions. Recognizing internal craze lines might indicate different etiologies or risk profiles compared to traditional craze lines, influencing preventive and therapeutic strategies in dental practice. Further research is needed to explore the prevalence, causes, and long-term impacts of internal craze lines.
Craze lines are a common occurrence in dental enamel, particularly in anterior teeth, and are often considered a natural part of the aging process [1,2]. They are generally confined to the enamel, do not extend into the dentin, and are typically regarded as nonstructural and benign [3-5]. Visible to the naked eye and more pronounced with magnification or plaque-disclosing dyes such as methylene blue, craze lines are often dismissed as aesthetic concerns [6]. They can occur on buccal surfaces, lingual surfaces, or both [7]. However, it is increasingly recognized that they may serve as early indicators of more significant structural issues within the tooth [8].
Historically, craze lines have been classified as superficial hairline cracks posing minimal risk to the overall tooth integrity [9,10]. These lines are usually the result of mechanical forces, thermal stresses, and normal wear and tear over time [11]. Since they do not typically involve the dentin, they are considered “nonstructural” and do not require intervention unless for cosmetic reasons [12-16]. Conversely, cracks penetrating the dentin are deemed “structural” and warrant treatment to prevent further damage or potential tooth fracture [4].
The clinical relevance of craze lines lies in their potential to serve as indicators of the overall structural integrity of a tooth. While traditionally viewed as non-threatening, the increased use of magnification in dental practice has revealed more about their characteristics and implications. According to the American Association of Endodontists, craze lines are classified among the five types of longitudinal tooth fractures, alongside fractured cusps, cracked teeth, split teeth, and vertical root fractures [17]. This classification underscores the importance of recognizing and understanding craze lines within the broader context of tooth fractures.
Craze lines can be stained to help distinguish them from deeper structural fractures. However, transillumination, while useful, can exaggerate the appearance of all cracks, making it difficult to differentiate between benign craze lines and more significant structural cracks. Subtle color changes indicating deeper issues can also be rendered invisible with this technique.
Currently, magnification and operating microscopes are becoming popular for precision in dentistry, aiding in observation and diagnosis [18,19]. Under magnification, craze lines comprise two types. One type, the proponent lines, reach the enamel surface and are sometimes tactile. The other type comprises sub-lines that do not reach the surface (Figure 1).

Figure 1: The photograph shows a detailed view of a tooth during restorative treatment for wear dentition. A central, long craze line runs from the cervical line to the incisal line, slightly stained and clearly visible. Additional lines, mainly on the sides, do not reach the surface but are revealed due to their angle and the lighting, appearing wider and more pronounced.
This study aims to differentiate between these two types based on their appearance and characteristics under visual, cross-sectional, and intraoral examination. This distinction enhances diagnostic accuracy, enabling better differentiation between purely aesthetic concerns and potential structural issues, highlighting the importance of advanced magnification tools in modern dental practice. By identifying internal craze lines as a distinct type of enamel anomaly, this study introduces a novel classification with important diagnostic and clinical implications.
Four anterior teeth were selected for this study from four patients, all of whom required tooth extraction due to advanced periodontal damage. The selection was based on the presence of both visible and internal craze lines in the teeth. These included one upper incisor, two lower incisors, and one lower canine. Prior to examination, the teeth were thoroughly cleaned to remove debris, remnants of the periodontal ligament, and tartar or calculus, ensuring clear and uncontaminated observation of the enamel structures. Verbal informed consent was obtained from all patients for the inclusion of their extracted teeth, clinical data, and images in this research and subsequent publication.
The objective was to conduct visual inspection and cross-sectional analysis to closely examine and differentiate between these two types of lines. Visual inspection in this study focused on examining traditional and internal craze lines within the enamel. Using the Euromex NexiusZoom (Evo) microscope from the Netherlands, equipped with black-and-white and twilight filters, researchers meticulously analyzed the dimensions and appearance of these lines. The lower canine presented both types of lines on its lingual and buccal surfaces, necessitating comprehensive photography using the ImageFocusAlpha program. Similarly, two lower incisors and one upper incisor exhibited lines exclusively on their buccal surfaces, selected for photographic documentation. Images were captured at various magnifications to ensure a thorough examination of traditional and internal craze lines.
For cross-sectional analysis, each of the four teeth was meticulously sectioned using a diamond bur under cooling to maintain optimal conditions. A diamond disk was specifically employed for precise sectioning. These sections were then examined under a stereo microscope equipped with filter options using the Euromex NexiusZoom (Evo) microscope from the Netherlands. This setup facilitated detailed observation and analysis of structural differences between traditional craze lines and newly discovered internal craze lines within the enamel. Additionally, the ImageFocusAlpha program associated with the microscope enabled the measurement of craze line lengths, enhancing the accuracy of evaluation and comparison across all specimens.
Microscopic examination of the selected anterior teeth revealed two distinct types of craze lines. The first type, the traditional craze line, extends from the Dentin-Enamel Junction (DEJ) to the surface of the enamel. These lines were observed as continuous cracks traversing the entire thickness of the enamel, from the outermost surface to the DEJ. They were clearly visible under the microscope, appearing as uninterrupted lines through the enamel.
Conversely, the newly identified internal craze lines originated at the DEJ but stopped midway through the enamel. These lines did not reach the enamel surface and were significantly shorter than traditional craze lines. They terminated within the enamel layer, marking a clear morphological distinction. Numerous instances of both types of cracks were found in the small sections of enamel studied, indicating their common occurrence.
Visual inspection
Before sectioning, visual inspection of the same teeth provided further insight into these craze lines (Figures 2-6).
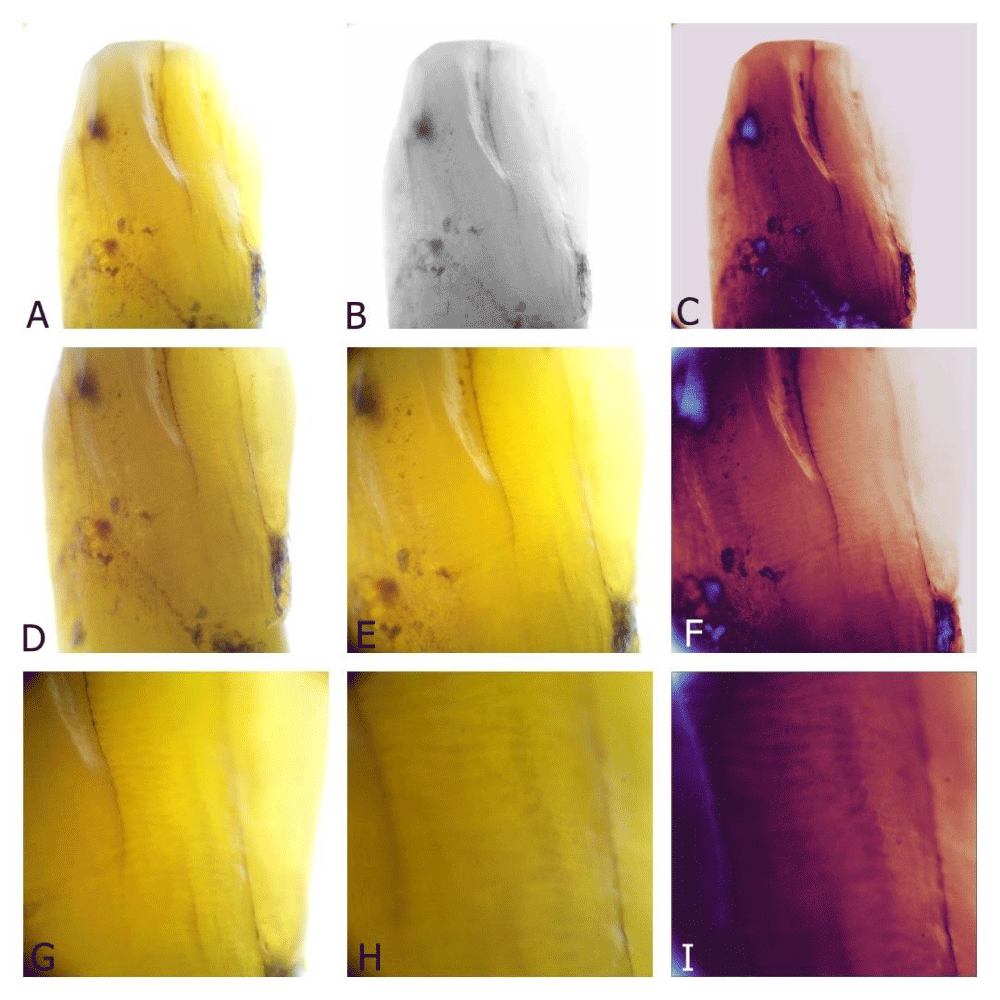
Figure 2: A. A lingual view of the lower canine, where distinct craze lines are prominently visible due to staining. This staining indicates a prolonged period of intraoral functioning, contributing to the formation and visibility of these lines. B. The same lingual view under a black-and-white filter. This high-contrast setting reveals the craze lines from another perspective, emphasizing their structure and presence on the tooth surface. C. Under a twilight filter, the defects in the lower canine become more pronounced. Even the internal craze lines, which are less noticeable under normal conditions, become more evident, illustrating the finer details of the tooth’s surface. D–G. Zoom into the craze lines to highlight their unique characteristics. The intricate patterns and pathways of these lines are captured in greater detail, showing their complexity. As the magnification increases, additional features invisible in a standard view become apparent, providing insight into the fine structure of these lines. A detailed examination showcases their depth and intersections across the enamel, enabling a closer examination of the patterns formed over time. H–I.150× magnification, revealing traditional and internal craze lines. The internal craze lines become more apparent, showing their characteristic of not reaching the outer surface of the enamel. Unlike continuous craze lines, internal craze lines are not continuous and appear segmented. The striae of Retzius act as a barrier between internal craze lines and the outer enamel, affecting only their appearance.
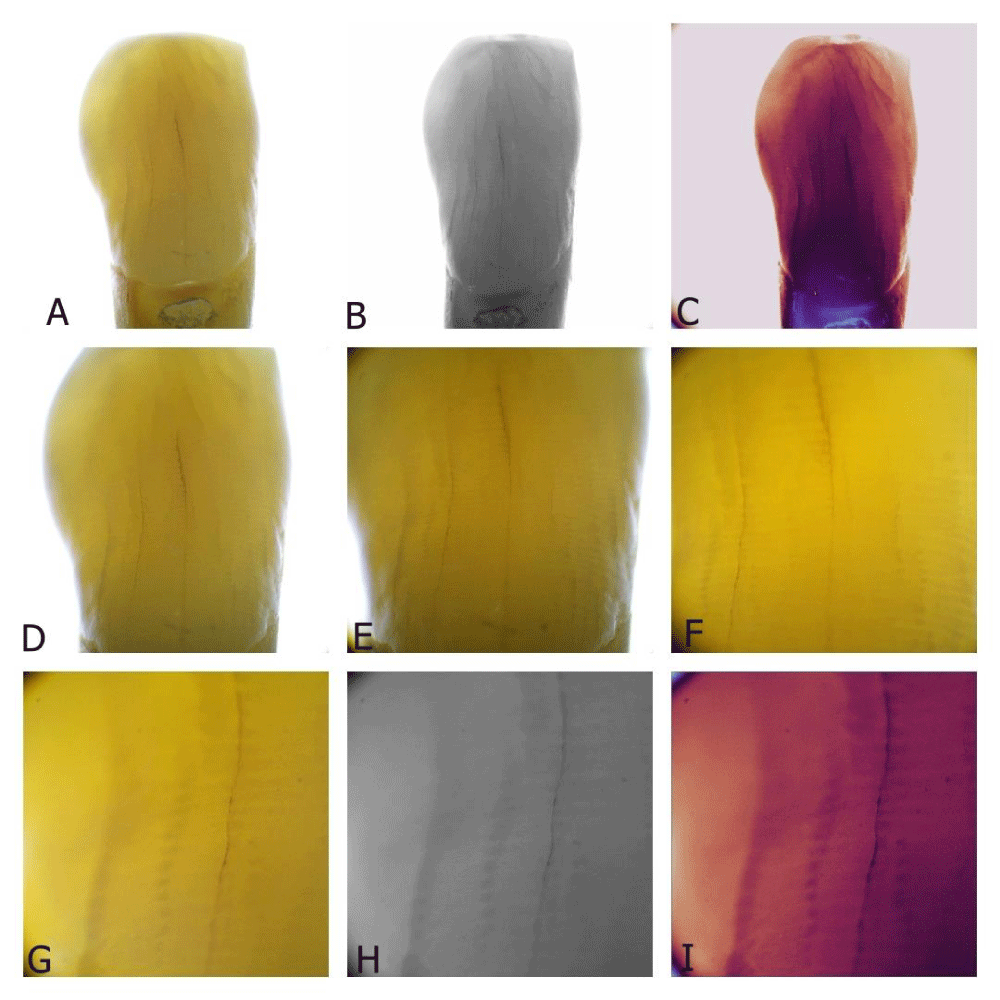
Figure 3: A. Buccal view of the lower canine. This view portrays the distinct characteristics and visibility of each craze line. B–C: The same buccal view with different filters. Each filter highlights specific and distinctive characteristics of the craze lines. Compared to internal craze lines, the traditional craze lines appear longer and darker, especially when stained and viewed under these filters. D–I: Zoom in on areas where the traditional and internal craze lines are proximal. This detailed view enables easier comparison between the two. It is clarified that internal craze lines appear thicker than traditional craze lines. This is not due to their actual width but how diagonal light reflects off them, creating the illusion of greater thickness. Additionally, the sectional view emphasizes the noticeable distinction of internal craze lines, highlighting their segmented appearance. y
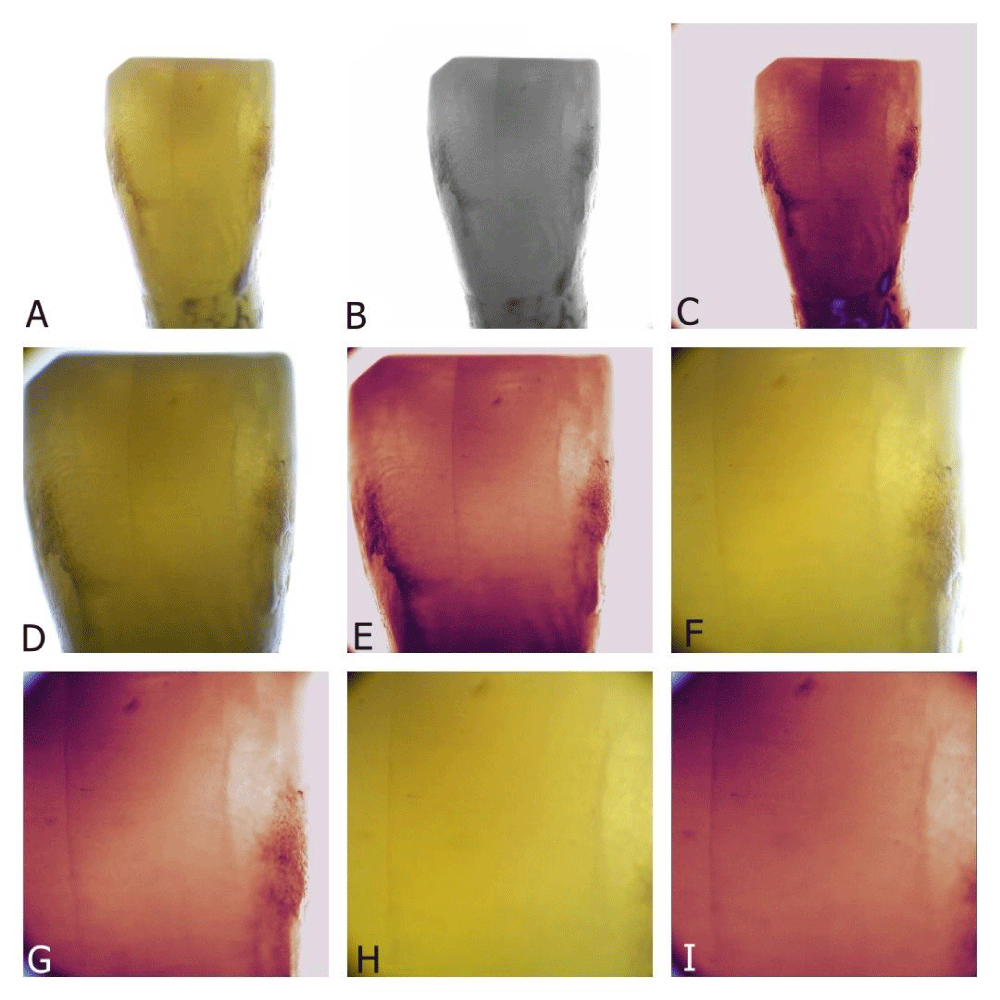
Figure 4: This series of images depicts the lower second incisor, captured in macro photography with various filters. A–B reveal superficial staining and subgingival tartar. However, the most striking features are the two craze lines. The first, a central craze line, runs vertically from the cervical third of the tooth to the incisal edge. This line is prominently visible across the images. The second, a shorter internal craze line, is located on the mesial side. This line appears to lie deeper within the tooth structure, suggesting it is beneath a superficial enamel layer. As the images progress from D to I, the camera gradually zooms in on these craze lines, ensuring both are within the frame for better comparison. Throughout all the images, the primary craze line remains clearly visible, while the secondary internal craze line appears to be situated deeper, enhancing the perception that a layer of enamel overlays it.
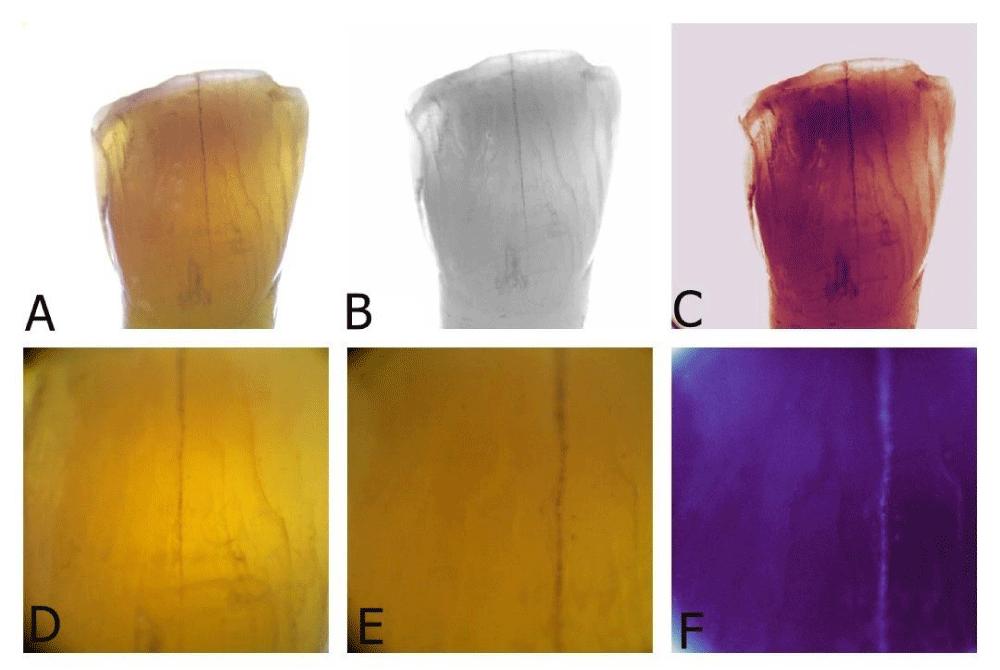
Figure 5: This series of images features a central incisor with a wear facet, where the incisal enamel is translucent. Across the three macro images (A–C), both the traditional and internal craze lines are distinctly visible. The use of filters enhances the prominence of the internal craze lines, making them even more dominant. The primary craze line is centrally located, extending from the cervical third of the tooth to the incisal edge. Surrounding this main line are numerous internal craze lines. The primary craze line is significantly longer, measuring more than double the length of the internal craze lines. As the images progress from D to F, a gradual zoom occurs, capturing both the primary and internal craze lines within the same frame for better comparison. With the filters applied, a noticeable contrast difference is visible between the primary craze line and the internal craze lines, highlighting the intricate details and varying depths of these features.
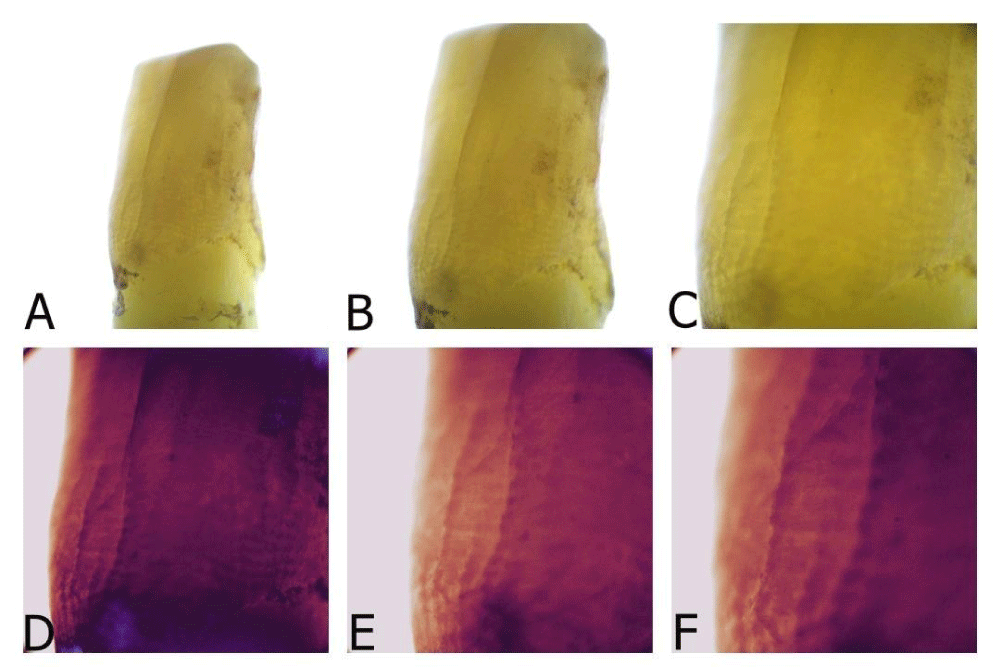
Figure 6: A–F This series of images showcases a lower incisor with a prominent craze line extending from the cervical region to the incisal edge. Initially, a direct buccal view reveals almost no visible internal craze lines. However, when viewed from a mesiobuccal angle, some internal craze lines become apparent in the cervical area. It appears that the primary craze line, which is more prominent at the incisal edge, transforms into internal craze lines near the cervical region. Zooming in on these features and using twin light filters makes all these defects distinctly visible, facilitating detection and diagnosis. The filters enhance the clarity of the primary craze line and the more subtle internal craze lines, highlighting the intricate details and making the imperfections more noticeable.
Traditional craze lines were highly exposed and easily visible, often appearing slightly darker than the surrounding enamel. These lines commonly extend from the cervical to the incisal edge of the tooth. Conversely, internal craze lines are presented differently. They were more subtle and typically required viewing from a specific angle to be observed. These lines appeared white and were usually visible only under certain lighting conditions and angles. They did not extend across the full height of the tooth and were typically 1–2 mm in length. Despite being less prominent, internal craze lines were found to be more numerous than traditional craze lines in the observed samples.
A detailed lingual view of the lower canine revealed distinct craze lines prominently visible due to staining (Figure 2).
This staining indicated a prolonged period of intraoral functioning, contributing to the formation and visibility of these lines. Viewing the same lingual surface under a black-and-white filter provided a high-contrast setting, revealing the craze lines from another perspective and emphasizing their structure and presence on the tooth surface. Under a twilight filter, even the internal craze lines, which were less noticeable under normal conditions, became more evident, illustrating the finer details of the tooth’s surface.
Zooming into the craze lines highlighted their unique characteristics. The intricate patterns and pathways of these lines were captured in greater detail, showing their complexity. As magnification increased, additional features not visible from a standard view became apparent, providing insight into the fine structure of these lines. This detailed examination showcased their depth and how they intersected across the enamel, enabling a closer view of the patterns formed over time.
At 150× magnification, traditional and internal craze lines became more apparent in all samples. Internal craze lines, unlike continuous craze lines, appeared segmented and did not reach the outer surface of the enamel. The striae of Retzius acted as a barrier between internal craze lines and the outer enamel, affecting only their appearance (Figures 2H-I, 3G-I).
Cross-sectional analysis
In vitro observations demonstrated that traditional craze lines extended from the outer enamel surface to the DEJ, while internal craze lines spanned from the mid-enamel or the border between the outer and inner enamel to the DEJ (Figures 7-11). This differentiation highlighted the structural variance between the two types of lines. Traditional craze lines are continuous lines running through the entire enamel thickness, whereas internal craze lines are confined within the inner enamel layer, not reaching the surface.
A cross-sectional view of the lower canine’s lingual side showcased the slice under various filters, highlighting four distinct craze lines (Figure 7). As the images zoomed in on these lines, the internal craze lines became fainter and more challenging to observe compared to the main craze line. Staining of the craze lines penetrated beyond the surface, indicating a deeper structural impact.
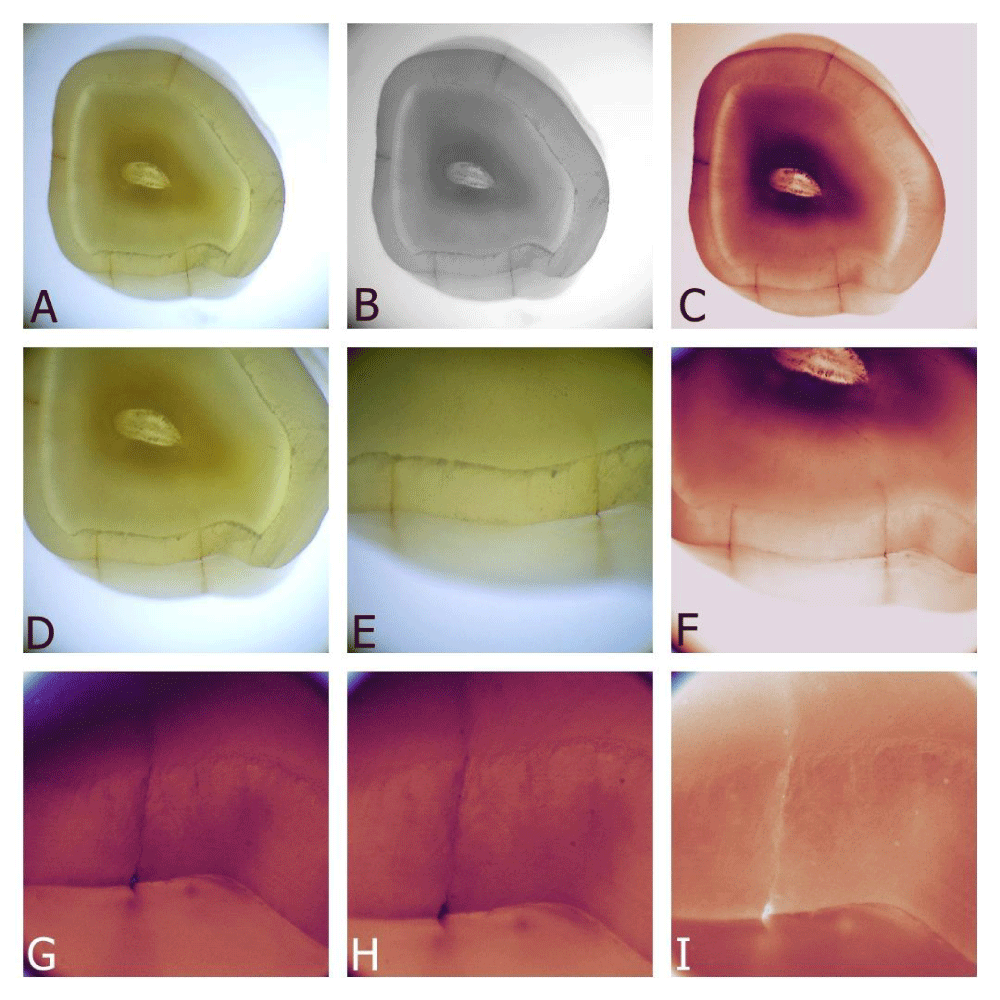
Figure 7: Cross-sectional view of the coronal part of the lower canine, focused on the lingual side. A–C display the same slice under different filters, highlighting various aspects of the craze lines. Four distinct craze lines are clearly visible. D–F zoom in on the two craze lines, where Fig 2 displays the images taken before slicing. G–I further zoom in on the rightmost craze line under different filters, revealing subtle internal craze lines, which are fainter and more challenging to observe than the main craze line. Notably, the staining of the craze lines is intriguing, as it penetrates beyond the surface into the craze line. The internal craze lines on this site are very short.
In another series, a buccal view of the lower canine revealed the distinct characteristics of each craze line (Figure 8A-I). Different filters highlighted specific characteristics, with internal craze lines appearing thicker due to light reflection despite their actual width. Zooming in on areas where traditional and internal craze lines were in close proximity enabled easier comparison, emphasizing the segmented appearance of internal craze lines (Figure 10A-I).
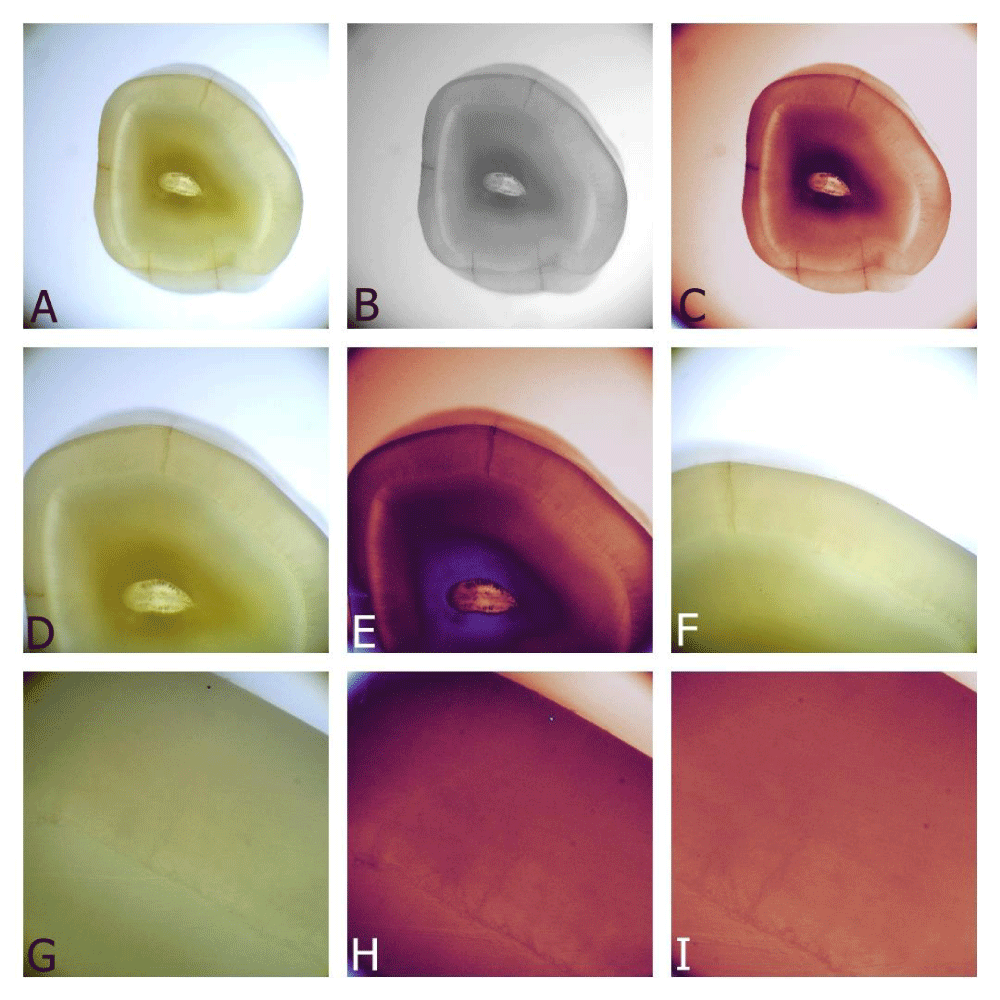
Figure 8: Zooming in on the buccal side of the same lower canine. A–C reveal the sliced piece under different filters to make the craze lines obvious, where only one craze line is visible on the buccal side. D–F zoom in on the area near the craze line to magnify the internal craze lines. G–I zoom in on the internal craze line, which is less visible than the main craze line but is present, starting from the DEJ and stopping within the inner enamel..
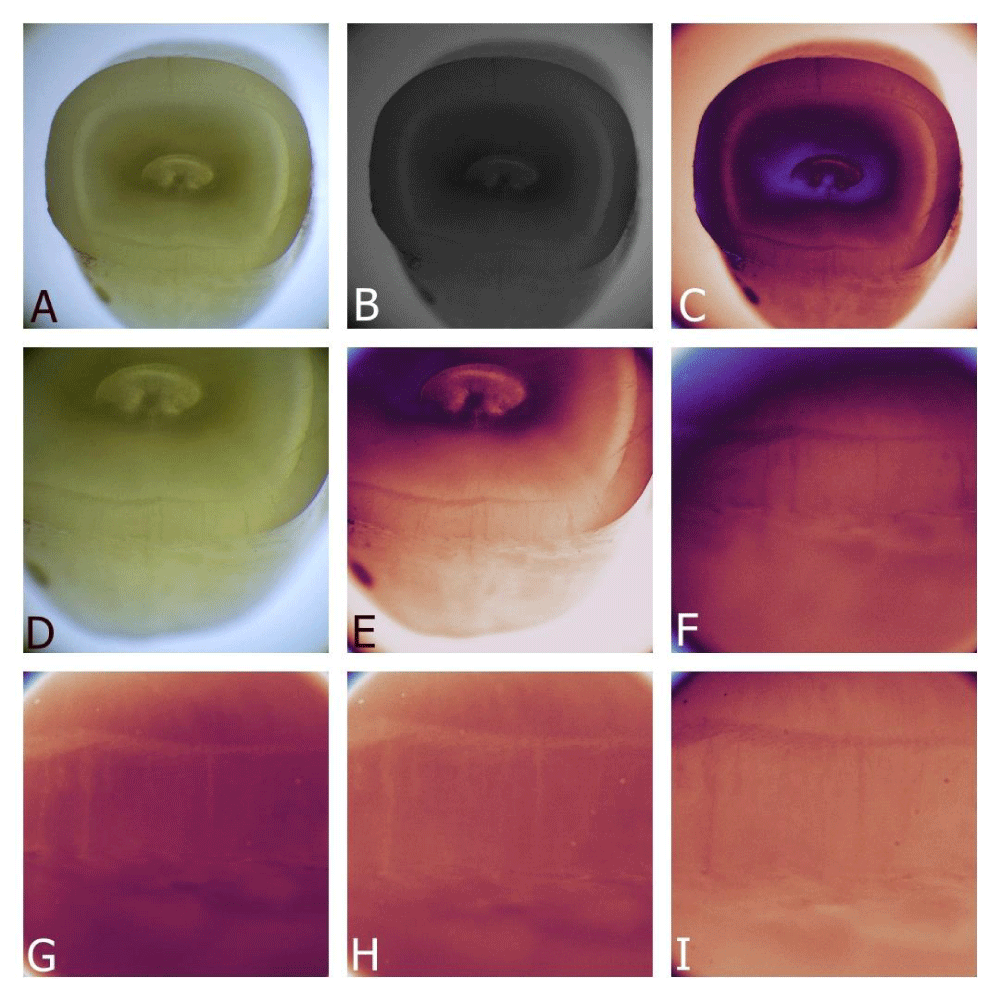
Figure 9: Sliced piece of a lower incisor, with the whole tooth shown in Fig 4. A–C highlight the lingual craze line under different filters. Since Fig 4 focuses on the buccal side, that side is examined here. D–F zoom in on the traditional and internal craze lines of the buccal side, making them more visible with the use of filters. G–I show both the traditional and internal craze lines in one frame, positioned near each other. The traditional craze line extends from the DEJ to the outer enamel surface, while the internal craze lines start at the DEJ but do not reach the outer enamel, giving them a unique intraoral appearance.
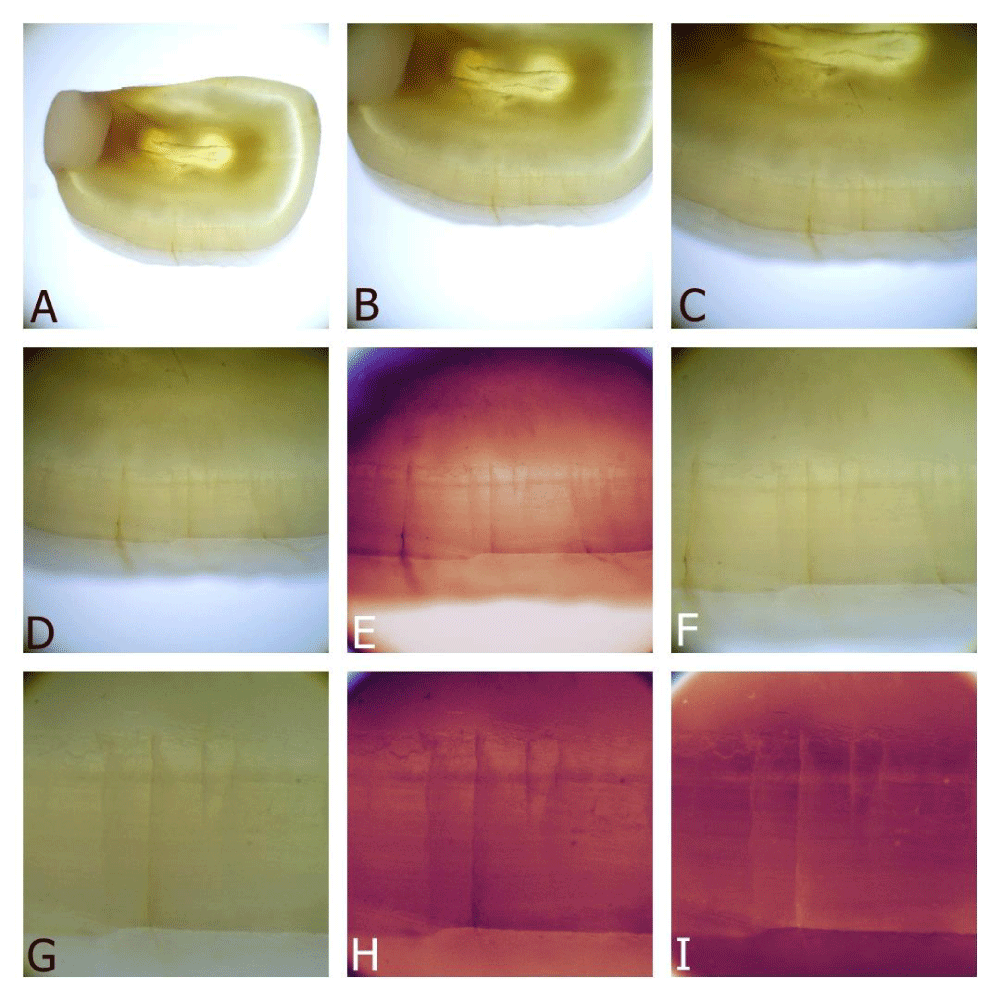
Figure 10: Cross-section of the upper central incisor, with the pre-slicing view shown in Figure 5. A. Although the composite restoration and wear on the palatal side have left almost no enamel, the focus is on the traditional and internal craze lines of the buccal side. B–F zoom in on both the traditional and internal craze lines. The staining of the craze line is more pronounced here, infiltrating deep into the craze, which should be considered during aesthetic treatments for patients. G–I show the same traditional and internal craze lines under different filters. Additionally, the striae of Retzius of the enamel are visible in these images, influencing the appearance of the internal craze lines.
The images of a lower incisor captured in macro photography (Figure 9A-C) showed both the traditional craze line and surrounding internal craze lines. The traditional craze lines, significantly longer and more prominent, were centrally located, while internal craze lines were shorter and positioned deeper within the tooth structure.
As the images progressed, the camera zoomed in on these craze lines, ensuring both were within the frame for better comparison. The use of filters enhanced the prominence of the internal craze lines, making them more dominant and highlighting their intricate details (Figure 9D-I).
A cross-section of the upper central incisor focused on the buccal side, with the pre-slicing view revealing pronounced staining and internal craze lines (Figures 5,10). Zooming in on these lines under different filters showed the striae of Retzius influencing the appearance of the internal craze lines. The staining of the craze line was more pronounced, infiltrating deep into the structure, which is crucial for aesthetic considerations in dental treatments.
The lower incisor images with internal craze lines visible near the proximal edges highlighted the segmented nature of these lines (Figures 6,11). Zooming in with twin light filters made all defects distinctly visible, enhancing detection and diagnosis. The filters improved the clarity of traditional and internal craze lines, showcasing their intricate details and making imperfections more noticeable.
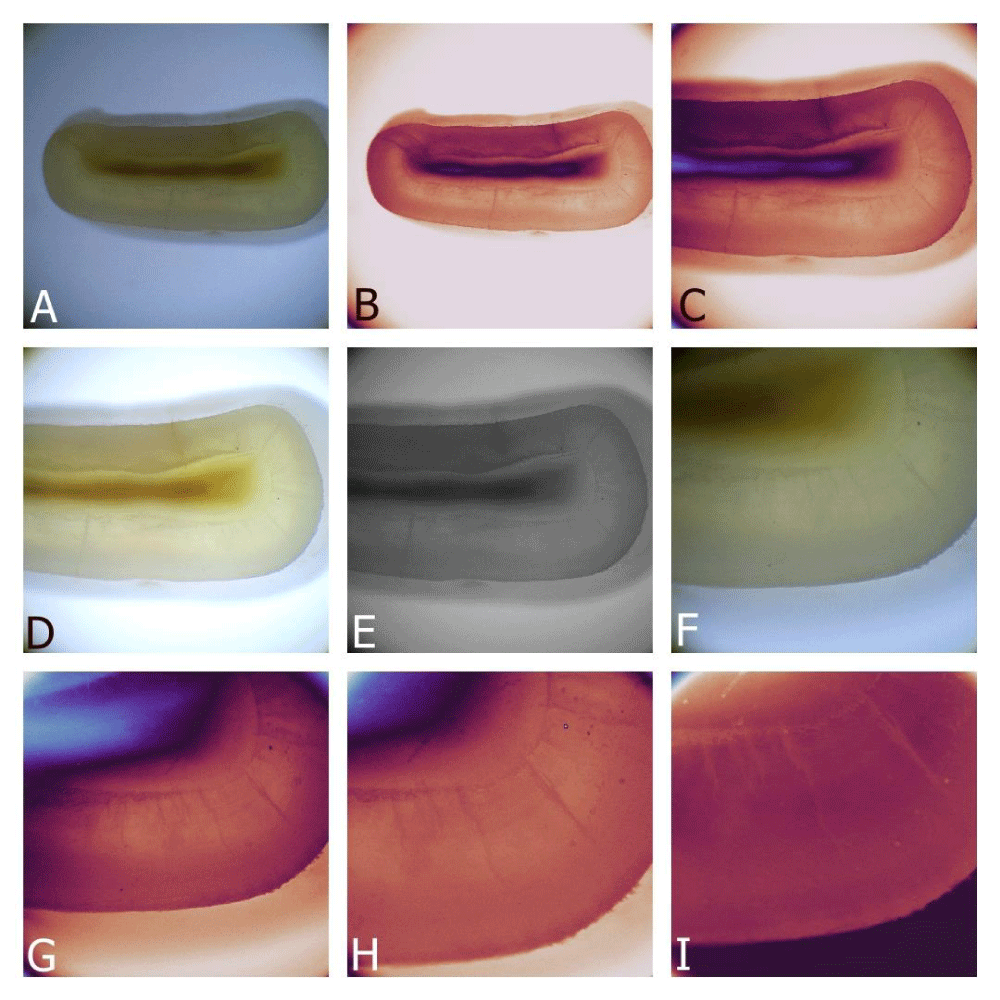
Figure 11: A–I Lower incisor with a craze line on the central buccal surface and internal craze lines visible near the proximal edges. The images focus on the internal craze lines, which are distant from the main craze line. Almost five internal craze lines of varying lengths are visible near the edge..
Microscopic examination of anterior teeth revealed two distinct types of craze lines: traditional craze lines, extending from the dentin-enamel junction (DEJ) to the enamel surface, and internal craze lines, which originate at the DEJ but terminate within the enamel. A study by Li, et al. [20] highlights the challenge of distinguishing these craze lines from more severe cracks, such as Enamel-Dentin (ED) cracks, using traditional methods [20]. The study utilized ICG-NIRF imaging to detect craze lines and ED cracks, demonstrating that ED cracks create a significant brightness contrast between the sides of the crack, while craze lines show little to no contrast. This imaging method could differentiate enamel-only cracks like craze lines from deeper ED cracks, offering a more reliable diagnostic tool than current surface-based practices, which often fail to detect crack depth or severity. Li et al.’s findings provide a modern context for comparing the traditional and internal craze lines observed in this study, highlighting advancements in imaging technologies that could improve crack detection and diagnosis.
Traditional craze lines, which extend from the DEJ to the enamel surface, are easily identifiable as continuous cracks traversing the entire enamel thickness. Intraorally, these lines appear darker than the surrounding enamel and can often be detected tactilely with a dental probe. However, internal craze lines originate at the DEJ but stop midway through the enamel, appearing as shorter, white lines requiring specific angles and lighting to be observed (Figure 12).
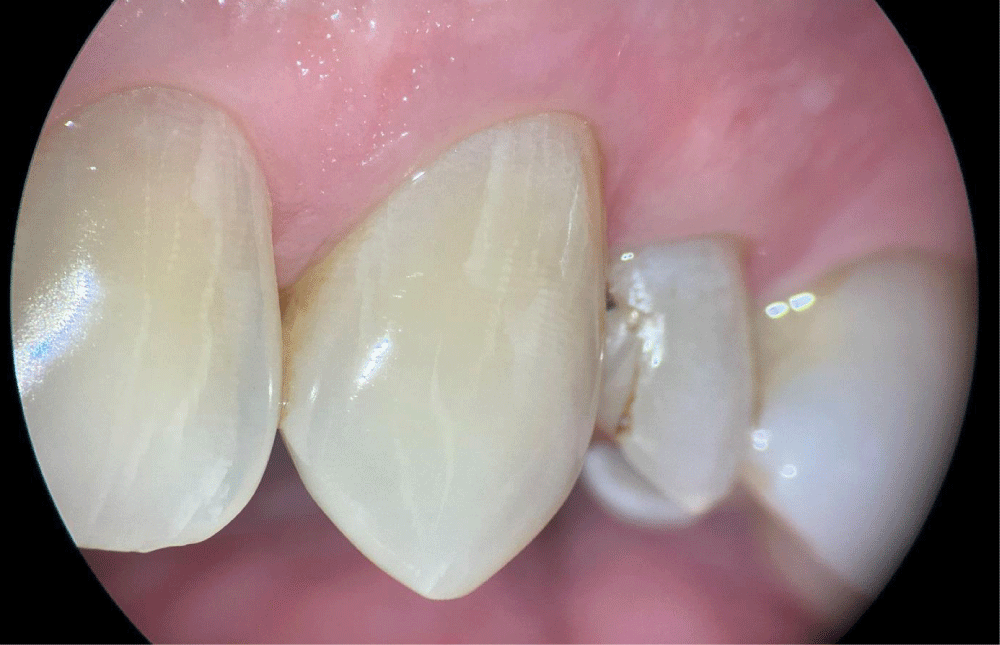
Figure 12: This image captures internal craze lines observed during a routine examination of a middle-aged patient. The photographs were taken using an operative microscope, with the angle from the mesial side enhancing the visibility of the lines. The short, thick, and chalky white lines are striking.
The advent of magnification and high-tech dental photography has become indispensable, particularly in restorative and endodontic treatments, enabling the detailed observation of enamel anomalies [4]. These technologies are now more commonly used, revealing many anomalies that were previously difficult to detect. However, transillumination is unsuitable for distinguishing between benign craze lines and more significant structural cracks, as it tends to amplify the appearance of all cracks (Figure 13) [21].
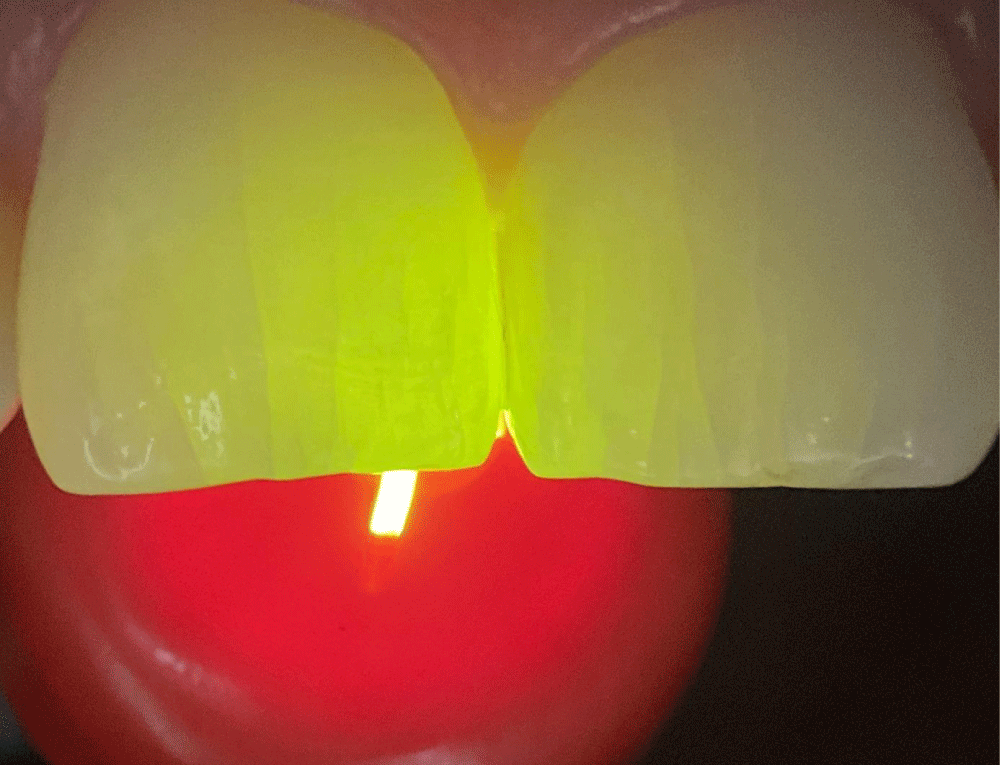
Figure 13: Transillumination is a well-established and reliable clinical method for detecting cracks and craze lines invisible under normal light. This technique can reveal most craze lines and their lengths with remarkable clarity. However, it still poses challenges in distinguishing between superficial and deeper internal craze lines.
In histological diagnosis, internal craze lines could be confused with other structures, such as enamel tufts. These tufts are hypomineralized regions comprising enamel rods and interprismatic substances that form due to the spatial adaptation of crystals within the enamel [22]. These natural defects originate from the DEJ and extend into one-third of the enamel thickness [23]. Enamel tufts, typically about 200 micrometers in height, are shorter and smaller than internal craze lines, which are about 1000 micrometers in height, appearing as wavy structures filled with organic material (Figure 14) [24]. They are considered intrinsic defects that can act as initiation points for internal cracks within the enamel. Although tufts can contribute to the formation of internal craze lines, they are also involved in stress distribution within the enamel, enhancing its mechanical properties despite being areas of weakness.

Figure 14: Measurement of the height of traditional and internal craze lines using the ImageFocusAlpha program shows that craze lines extend through the entire thickness of the enamel in that region, whereas internal craze lines are only about 1000 micrometers in height.
Although the origin of enamel tufts has not been clearly established, a correlation exists between internal craze lines, age, and parafunctional habits. These defects are more frequently observed in middle-aged and older patients [24].
In restorative dentistry, the ability to distinguish between traditional and internal craze lines has significant implications. For example, traditional craze lines can often be masked or cleaned to remove stains using air particle abrasion and resin materials. This is not the case with internal craze lines, which lie deeper within the enamel and are more challenging to mask effectively. Recognizing the presence of internal craze lines allows practitioners to make informed decisions about the depth of intervention required. In minimally invasive restorative treatments aimed at aesthetic improvements, understanding that internal craze lines are embedded deeper in the enamel means that removing or masking these lines may require sacrificing more of the outer enamel. This knowledge helps dental professionals balance the aesthetic outcomes with preserving tooth structure.
The striae of Retzius, which marks changes in enamel growth and content, significantly influences the appearance of internal craze lines (Figure 15). While they do not act as physical barriers, they affect the visibility and apparent segmentation of internal craze lines. The striae of Retzius are visible under different filters and contribute to how internal craze lines are perceived, differentiating them from the continuous nature of traditional craze lines.
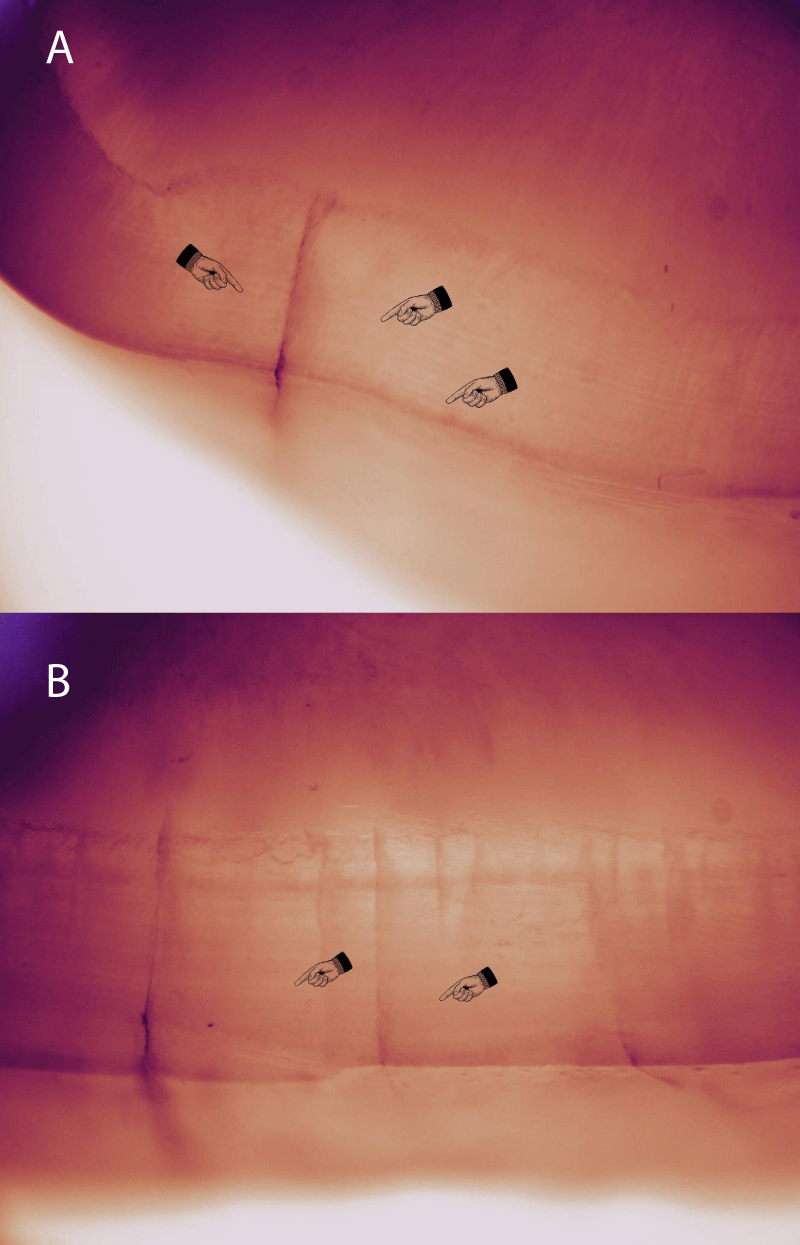
Figure 15: A,B: In the cross-sectional analysis of the examined teeth, the striae of Retzius are remarkably prominent. These lines are also clearly visible on visual inspection and directly influence the appearance of internal craze lines.
Although internal craze lines are not immediately indicative of deeper structural damage, their presence could compromise the enamel’s resilience to ongoing stress, potentially leading to the propagation of deeper cracks or fractures. This could influence treatment decisions in restorative dentistry, as practitioners must weigh the risks of leaving these defects untreated against the potential harm that could arise from more invasive interventions. Monitoring internal craze lines over time, especially in patients with high occlusal forces or habits such as bruxism, could be critical in preventing progression into more significant enamel or dentin damage.
Additionally, the knowledge of internal craze lines aids in managing patients presenting with these features. Knowing that internal craze lines are more numerous yet less conspicuous than traditional craze lines underscores the need for thorough examinations using magnification. This ensures that all structural anomalies are accounted for during diagnosis and treatment planning.
Regarding the limitations of this study, one important factor is the reliance on magnification and high-tech dental photography for the detection and analysis of internal craze lines. While these technologies are becoming more widely available, they may not be universally accessible in all clinical settings, limiting the broader applicability of the findings. Additionally, this study does not explore the long-term progression of internal craze lines or their potential impact on tooth longevity, focusing instead on structural characteristics rather than clinical outcomes. Future research should address these gaps by conducting longitudinal studies to assess the long-term behavior of internal craze lines across diverse patient populations. Investigating the conditions that contribute to their formation, such as the role of enamel tufts, could offer valuable insights into preventive strategies and help develop treatment protocols aimed at halting the progression of these internal defects. This knowledge would ultimately improve clinical outcomes and provide clearer guidance for clinicians when managing internal craze lines.
Future research must focus on exploring the prevalence, causes, and long-term impacts of internal craze lines. Investigating the conditions leading to their formation, such as the role of enamel tufts, could provide insights into preventive strategies and improve clinical outcomes.
The identification of internal craze lines within human enamel holds significant clinical implications. Differentiating between traditional craze lines, which extend from the DEJ to the enamel surface, and internal craze lines, which terminate midway through the enamel, can enhance diagnostic accuracy and inform treatment decisions. Recognizing internal craze lines may indicate different etiologies or risk profiles compared to traditional craze lines, thereby influencing preventive and therapeutic strategies in dental practice. The identification of internal craze lines as a novel category enhances understanding of enamel integrity and provides a foundation for improved diagnostic and treatment approaches. Further research is required to explore the prevalence, causes, and long-term impacts of internal craze lines, ultimately improving the understanding and management of these dental anomalies.
The author declares no financial interest in any of the mentioned devices. While writing a book on cracked teeth, the author encountered these unique internal craze lines, which had not been previously documented. This discovery prompted a deeper investigation into their characteristics and implications, enriching the understanding of dental enamel fractures.
The author hereby declare that I have utilized Artificial Intelligence (AI) tools in the development of this manuscript. Specifically, the following AI tools were used: ChatGPT, an AI language model, was employed for grammar and spelling checks, as well as for drafting and refining sections of the text. While AI tools were used to assist in the production of content or data analysis, I have personally reviewed and ensured the accuracy, integrity, and originality of the final work. I take full responsibility for the content presented in this manuscript, including any intellectual contributions made by AI tools.
- Yahyazadehfar M, Zhang D, Arola D. On the importance of aging to the crack growth resistance of human enamel. Acta Biomater. 2016;32:264-274. Available from: https://doi.org/10.1016/j.actbio.2015.12.038
- Oh C, Lee H, Kim J, Lee JH, Nguyen T, Kim KH, et al. The influence of age and orthodontic debonding on the prevalence and severity of enamel craze lines. J Am Dent Assoc. 2023;154:601-609. Available from: https://doi.org/10.1016/j.adaj.2023.04.004
- Lynch C, McConnell R. The cracked tooth syndrome. J Can Dent Assoc. 2002;68:470-475. Available from: https://pubmed.ncbi.nlm.nih.gov/12323102/
- Clark D, Sheets C, Paquette J. Definitive diagnosis of early enamel and dentin cracks based on microscopic evaluation. J Esthet Restor Dent. 2003;15:391-401. Available from: https://doi.org/10.1111/j.1708-8240.2003.tb00963.x
- Davich M. Clinical detection and decision-making considerations for cracked teeth. Endod Therapy. 2004;4:4–7. Available from: https://sitefiles.tdo4endo.com/files/webid0186/imagesdr/200402ENDO_DavichCrackedTeeth.pdf
- Ghorbanzadeh A, Aminifar S, Shadan L, Ghanati H. Evaluation of three methods in the diagnosis of dentin cracks caused by apical resection. J Dent (Tehran). 2013;10:175-185. Available from: https://pubmed.ncbi.nlm.nih.gov/23724218/
- Alsolaihim AN, Alsolaihim AA, Alowais LO. In vivo and in vitro diagnosis of cracked teeth: A review. J Int Oral Health. 2019;11:329-333. Available from: https://journals.lww.com/jioh/fulltext/2019/11060/in_vivo_and_in_vitro_diagnosis_of_cracked_teeth__a.1.aspx
- Bajaj D, Nazari A, Eidelman N, Arola DD. A comparison of fatigue crack growth in human enamel and hydroxyapatite. Biomater. 2008;29:4847-4854. Available from: https://doi.org/10.1016%2Fj.biomaterials.2008.08.019
- Abou-Rass M. Crack lines: The precursors of tooth fractures — their diagnosis and treatment. Quintessence Int. 1983;4:437-447. Available from: https://pubmed.ncbi.nlm.nih.gov/6574554/
- Ellis SG. Incomplete tooth fracture—proposal for a new definition. Br Dent J. 2001;190:424-428. Available from: https://www.nature.com/articles/4800873
- Xu HH, Kelly JR, Jahanmir S, Thompson VP, Rekow ED. Enamel subsurface damage due to diamond tooth-preparation. J Dent Res. 1997;76:1698-1706. Available from: https://doi.org/10.1177/00220345970760101201
- Mamoun JS, Napoletano D. Cracked tooth diagnosis and treatment: An alternative paradigm. Eur J Dent. 2015;9:293–303. Available from: https://doi.org/10.4103/1305-7456.156840
- Johnson R. Descriptive classification of traumatic injuries to the teeth and supporting structures. J Am Dent Assoc. 1981;102:195-197. Available from: https://doi.org/10.14219/jada.archive.1981.0112
- Andreasen JO. Traumatic Injuries of the Teeth. 2nd ed. Copenhagen: Munksgaard; 1981:19.
- Caufield JB. Hairline tooth fracture: A clinical case report. J Am Dent Assoc. 1981;102:501-502. Available from: https://doi.org/10.14219/jada.archive.1981.0145
- Kahler W. The cracked tooth conundrum: Terminology, classification, diagnosis, and management. Am J Dent. 2008;21:275-282. Available from: https://www.amjdent.com/Archive/ReviewArticles/2008/Kahler%20AJD%2010-08.pdf
- American Association of Endodontics. Cracking the cracked tooth code. Endod Colleagues Excell Newsl. 1997.
- Bud M, Jitaru S, Lucaciu O, Korkut B, Dumitrascu-Timis L, Ionescu C, et al. The advantages of the dental operative microscope in restorative dentistry. Med Pharm Rep. 2021;94:22-27. Available from: https://doi.org/10.15386/mpr-1662
- Christensen GJ. Magnification in dentistry: Useful tool or another gimmick? J Am Dent Assoc. 2003;134:1647-1650. Available from: https://doi.org/10.14219/jada.archive.2003.0111
- Li Z, Holamoge YV, Li Z, Zaid W, Osborn ML, Ramos A, Miller JT, Li Y, Yao S, Xu J. Detection and analysis of enamel cracks by ICG-NIR fluorescence dental imaging. Ann N Y Acad Sci. 2020 Sep;1475(1):52-63. Available from: https://doi.org/10.1111/nyas.14374
- Mathew S, Thangavel B, Mathew CA, Kailasam S, Kumaravadivel K, Das A. Diagnosis of cracked tooth syndrome. J Pharm Bioallied Sci. 2012;4(Suppl 2). Available from: https://doi.org/10.4103%2F0975-7406.100219
- Palamara J, Phakey PP, Rachinger WA, Orams HJ. Ultrastructure of spindles and tufts in human dental enamel. Adv Dent Res. 1989;3:249-257. Available from: https://doi.org/10.1177/08959374890030022601
- Hudson AL. A study of the effects of mesiodistal reduction of mandibular anterior teeth. Am J Orthod. 1956;42:615-624. Available from: https://doi.org/10.1016/0002-9416(56)90103-8
- Desoutter A, Panayotov I, Cuisinier F, Carayon D. Human tooth enamel tuft drapes revealed by microtomography. Arch Oral Biol. 2022;141:105487. Available from: https://doi.org/10.1016/j.archoralbio.2022.105487